Guest contribution:
 Article series on the subject of state-of-the-art mycology in dermatology,
Article series on the subject of state-of-the-art mycology in dermatology,
4th article

by Prof Hans-Jürgen Tietz, Director of the Institute of Fungal Diseases in Berlin, Germany
According to Professor Hans Rieth, the unforgotten master of mycological entertainment, the clinical eye is often a relative of the evil eye. He described the problem of incorrect visual diagnoses, which still occurs today. Around 30% of patients who go the doctor believing they have a fungal infection, in fact have a non-infectious nail disease. In our practice this sometimes occurs with four out of five patients a day. The misjudgement often follows the same storyline:
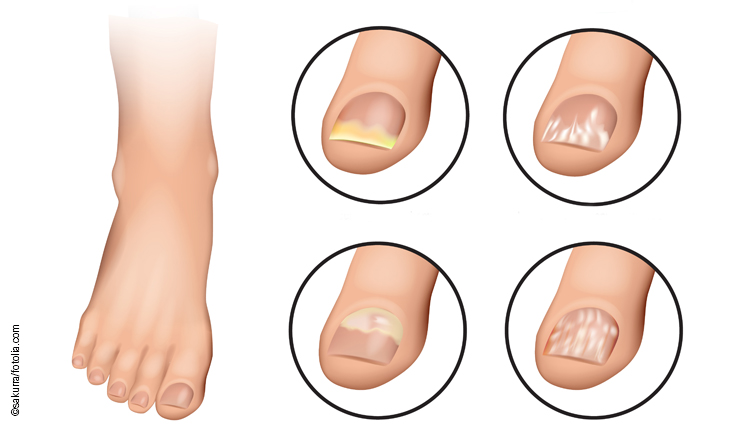
“I saw an advert on TV for a fungal product and went to the pharmacy because of my nail fungus. They said they could help. But nothing worked, and now I have to see a doctor as they’ve tried everything. The doctor said it’s not a fungus. But I am frustrated and have doubts about the competence of the doctor. It can’t be anything else, can it? But what if it isn’t a fungus?” There is in fact a huge reservoir of differential diagnoses, which the general public doesn’t want to believe. Most frequently ram’s horn or claw-shaped nails are confused with a fungal infection, as in the case of our young patient in Fig. 1.

In contrast to mycoses, such nails are rock hard. You can hardly cut them. Rudolf Virchow, the famous pathologist and renowned politician, who is still highly esteemed in Berlin to this day, referred to the pathological cornification of the nail as onychogryphosis.
It is often genetic: oh yes, my Gran had nails like this as well. Occurrence in young children also argues against mycosis, which has its first peak between the ages of 7 and 12 years.
Despite the clear visual diagnosis, we carried out diagnostic tests at the request of the family. The referring paediatrician requested a PCR as proof. Our suggestion was to perform a culture, and, if the result was negative and after consultation with the family, to do a genetic test of the chippings remaining on the medium. The PCR was negative as expected, but was received with goodwill by the family. The child was no longer infectious. And the prospect of treatment with a nail varnish containing a high concentration of urea, which would soften the nail so that it could be better cut, was welcomed. However, most effective is a long-term podological treatment. Surgery is only required in extreme cases, such as in horseshoe crab-like nail growth anomaly, which is also often mistaken for mycosis.
Nail psoriasis is also often confused with mycosis. This affects in particular the phenomenon of white nail. Would you not have suspected mycosis in patients A and B in Fig. 1? It is an increasing problem, which occurs particularly often in patients with hypertension when they change from original drugs to generics. In these cases, PCR is the strongest microbiological argument against mycosis due to its outstanding sensitivity. It convinces most patients. After all, in corona times you can often only travel from A to B with a negative gene test. Whether changing to a different drug results in healthy nails again is another important question, but an often helpful idea.
Our conclusion: A negative result has important diagnostic significance – even in mycology. And it fits with the aphorism of Hans Rieth, who wants to tell us that it is better to have a negative result than no microbiological diagnostic information or relying only on the clinical eye.
The legendary Hans Rieth was the inventor of the DHS system which is still popular today. He travelled with his myco-mobile around Germany to train doctors. He was for decades an independent honorary scientist at the University of Hamburg and worked at the frontline running a GP practice in Wandsbek —with wisdom and humour, as shown by the citations here.
The articles under the rubric “Guest contribution” only reflect the views of the respective authors. Responsibility for the legality and content of the articles lies solely with the authors. EUROIMMUN does not assume liability for the completeness, accuracy and currentness of the information provided.